
OLSSON'S IS CLOSED
Thank you to all our loyal customers who supported us for 36 years
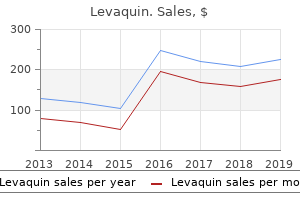
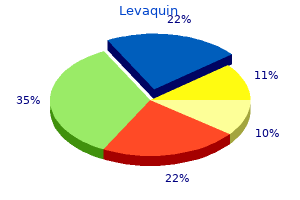
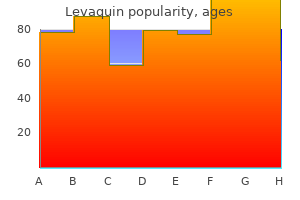
"Purchase online levaquin, medications vertigo".
By: U. Sivert, M.A.S., M.D.
Medical Instructor, New York Institute of Technology College of Osteopathic Medicine at Arkansas State University
Gunning splints) symptoms zoloft overdose discount 250mg levaquin visa, external frame and pin fixation symptoms internal bleeding cheap levaquin 750mg without a prescription, and various forms of interdental wiring medications held for dialysis purchase levaquin 750 mg amex. These methods rely on secondary bone healing treatment 8 cm ovarian cyst buy levaquin 250mg lowest price, but have limited application in trendy follow, because of the delayed return of operate and higher rates of infection, malunion, nonunion and malocclusion. This led to the event of open discount and internal fixation methods, which provides anatomical reduction and stabilization, in turn optimizing primary bone healing. One of the sooner forms of inside fixation was using transosseous wires, a semi-rigid type of fixation, which was an effective technique for its time, and is occasionally still employed. In the 1960 and Nineteen Seventies, this technique was changed with the appearance of plates and screws. These early plating techniques had been first adopted from orthopaedic experience with the therapy of lengthy bone fractures. However, large compression plates, which used bicortical screws that had been positioned along the inferior border of the mandible splayed the superior side of the fracture. Compression plates apply drive to areas of the mandible that are already underneath biomechanical compression. Eccentric dynamic compression plates have been then developed to attempt to counteract these distaction forces, however had been too cumbersome and approach delicate. More latest advancements in plating techniques have provided many alternative forms of plating expertise to the surgeon including nonlocking plates, threaded locking plates, tapered locking plates, bicortical and monocortical fixation, inflexible and semi-rigid plates. The targets of treatment must be as follows: anatomic reduction and stabilization of fractures; preservation of facial dimensions; set up and preserve the occlusion; early return to operate; avoidance of an infection. Understanding these objectives is paramount and the surgeon must weigh the risks in opposition to the advantages of the proposed management. The objective of this chapter is to provide the clinician with an outline of the advancements made in maxillofacial fixation and the types of methods obtainable. The affected person is placed into his premorbid occlusion upon the ultimate tightening of the intra- and interarch wires. They provide a versatile means of directing vectors of forces with a V�W pattern of crossbracing, to assist in fracture discount and re-establishment of the premorbid occlusion. The top of contour place and contacts within the major dentition could stop the application of circumdental wires. Many clinicians elect to use them based mostly on a decreased risk of penetrating damage for the person, ease of placement with shorter working room time, decreased trauma to the periodontium, convenience of maintaining oral hygiene, and the flexibility to use them each intraoperatively and post-operatively, corresponding to with guiding elastics. Because they required a drilled gap for placement, there have been concerns about suboptimal placement and root injury that occurred during placement. The second technology self-drilling/selftapping screws improved tactile feedback, limiting the possibility of root damage. The producer recommends putting screws above the basis apices; nevertheless, the creator has found that subapical placement led to mucosal overgrowth complicating their removal. Instead the screws ought to be positioned in a bicortical style between the roots at the level of the mucogingival junction. It is recommended, if potential, to acquire a panorex film previous to placement of the screws so as to consider the basis morphology. When possible, no less than one screw should be positioned proximal and distal to the fracture. However, a quantity of screws may be positioned to direct the vectors of the interarch wires appropriately, which in flip aids in fracture discount and stabilization. Recent reviews have illustrated a number of inherent risks and limitations which include root damage, screw loosening, screw shearing and aspiration. The self-drilling feature presents a larger degree of tactile suggestions during placement, permitting the operator to change insertion location before root injury occurs. However, by way of the developments made with rigid fixation, in addition to microvascular reconstructive surgery, this technique has waned in its use. Once soft tissue stabilization is achieved, the definitive restore can happen and the exterior fixation removed. First-generation external fixators utilized transcutaneous bicortical pins (placed alongside the inferior border) which had been then bridged by filling an endotracheal tube with acrylic resin.
In selected situations symptoms 3 days after conception generic levaquin 250 mg online, stereolithographic fashions might aid in therapy planning treatment 10 purchase levaquin without a prescription, osteotomy location and gadget contouring symptoms magnesium deficiency order discount levaquin online. In cleft maxilla patients medicine 75 yellow purchase discount levaquin on-line, pre-operative speech evaluation with nasopharyngeal airflow research and/or fibreoptic nasopharygoscopy is important to determine borderline or frank velopharyngeal incompetence which may worsen with distraction. All scientific and diagnostic instruments are utilized to plan out the correct 3D distraction vector choice and distance of distraction. Maxillary distraction osteogenesis device choice is predicated on obtainable bone stock, ease of application, distance of distraction osteogenesis and talent to adjust the distraction vector submit system placement. Intraoral boneborne devices have many advantages including good device 668 Maxillary distraction osteogenesis by intraoral and extraoral strategies stability and longer consolidation instances, though extraoral gadgets with cranial stabilization, in selected cases, have advantages such as longer distraction distances and talent to regulate distraction vector, but usually have shorter consolidation occasions. Occasionally, sufferers with extreme maxillary retrognathism with sleep apnoea have tracheostomy tubes which could be utilized for inhalational anaesthesia. After establishing common anaesthesia and administering appropriate antibiotic prophylaxis, consideration is directed to the maxillary vestibule the place native anaesthetic 2 per cent lidocaine 1/100 000 epinephrine is infiltrated within the deliberate area of incision. Toxic dosages should be averted, notably in paediatric sufferers or these sufferers with cardiac anomalies. After allowing suitable time for haemostasis, a vestibular incision is made a minimum of 5 mm above the attached gingiva from zygoma to zygoma. It is fascinating to depart significant labial connected gingiva pedicled to the maxilla. Osteotomy location is predicated on the need for sufficient bone above and under the osteotomy website for software of the bone-borne distraction units. At this level, the extent of the osteotomy is marked with a 701 tapered fissure bur or with a reciprocating saw. All bone cuts or osteotomies are made with sufficient soft tissue retraction and copious saline irrigation. It is advisable at this time to contour and safe the left and right bone-borne distraction devices with two screws above and beneath the osteotomy web site. It is essential to have the vector of the distraction device near the sagittal plane and never convergent. The osteotomy location might have to be greater in younger patients where the growing canine enamel are unerupted. External maxillary devices utilize a tooth-borne component which permits higher flexibility of osteotomy location. A Frier elevator is used to strip the nasal mucosa from the inferior and lateral facet of the lateral nasal wall to the posterior extent of the nasal wall. A periosteal retractor is placed along the lateral nasal wall to prevent tearing of the tissues. Next the anterior nasal spine is dissected free and initial area of the attachment of the nasal septal cartilage to the maxilla is freed up. The nasal mucosa is stripped from the floor of the nasal cavity and the inferior aspect of septal cartilage. It is essential to place the osteotome near the inferior facet of the pterygomaxillary junction and angled inferiorly in Operative technique 669 (a) (b) 10. The operating surgeon controls the pterygoid osteotome and locations a finger on the palatal aspect of the pterygomaxillary junction, while the surgical assistant strikes the osteotome with the mallet. Subsequently, the maxilla is digitally down-fractured with stress on the anterior maxilla and midface. If issue is experienced in mobilizing the maxilla, recheck all osteotomy cuts, and if needed the Rowe disimpaction forceps may be positioned on the nasal floor below nasal mucosa and on the onerous palate to unlock the maxilla. Copious saline irrigation is carried out, haemostasis is obtained and tissue are closed in a two layer trend with 3/0 vicryl interrupted horizontal mattress sutures in the muscle periosteum layer. The mucosal incision is closed with 4/0 monofilament nylon horizontal mattress sutures for wound eversion then 4/0 chromic gut operating suture for watertight closure. The incision might have considerable pressure on it throughout lengthy distraction distances. It is typical to have the gadget activation arm exit by way of the incision line or by way of a separate transmucosal stab incision depending on gadget place. Three to four screws per facet is desirable, 2�4 cm above the helix of the ear, avoiding the skinny bone of the temporal fossa. An osteotomy is made with the reciprocating noticed from the zygoma to the piriform rim at the acceptable degree. With the Langenback toe out retractor positioned to the pterygomaxillary junction, the osteotomy is carried out posteriorly and inferiorly again to the pterygomaxillary junction.
As the primordial coronary heart bends treatment 8th feb cheap 250mg levaquin amex, the atrium and sinus venosus appear dorsal to the truncus arteriosus symptoms 4 days after ovulation buy levaquin 250mg without a prescription, bulbus cordis medicine 6 times a day buy generic levaquin 750 mg on line, and ventricle medicine world nashua nh order levaquin online now. By this stage, the sinus venosus has developed lateral expansions, the right and left horns of the sinus venosus. The heart is initially suspended from the dorsal wall by a mesentery (double layer of peritoneum), the dorsal mesocardium. B, Ventral view of the guts and pharyngeal arch arteries at roughly 35 days. The ventral wall of the pericardial sac has been eliminated to show the center within the pericardial cavity. The endocardial cushions develop from a specialized extracellular matrix (intracellular substance of a tissue) related to the myocardium in addition to neural crest cells. Its formation is related to the expression of remodeling development factor-2 and bone morphogenetic proteins 2A and 4. B, Frontal section of the guts through the fourth week (approximately 28 days) exhibiting the early look of the septum primum, interventricular septum, and dorsal endocardial cushion. C, Frontal part of the guts (approximately 32 days) displaying perforations in the dorsal part of the septum primum. D, Frontal section of the center (approximately 35 days), displaying the foramen secundum. The arrow signifies the flow of well-oxygenated blood from the proper to the left atrium. The septum primum grows towards the fusing endocardial cushions from the roof of the primordial atrium, partially dividing the atrium into proper and left halves. As this curtain-like muscular septum develops, a big opening-the foramen primum-forms between its free edge and the endocardial cushions. This foramen allows shunting of oxygenated blood from the proper to the left atrium. Before the foramen primum disappears, perforations produced by apoptosis (programmed cell death) appear in the central part of the septum primum. As the septum fuses with the endocardial cushions, obliterating the foramen primum. This foramen ensures continued shunting of oxygenated blood from the right to the left atrium. The septum secundum grows from the muscular ventrocranial wall of the atrium, immediately adjacent to the best of the septum primum. As this thick septum grows in the course of the fifth and sixth weeks, it gradually overlaps the foramen secundum in the septum primum. The septum secundum types an incomplete partition between the atria: the opening within the foramen secundum-oval foramen (foramen ovale). The remaining part of the septum, hooked up to the endocardial cushions, forms the valve of the oval foramen. It also prevents the passage of blood in the reverse direction because the septum primum closes towards the comparatively inflexible septum secundum. After start, the oval foramen functionally closes due to larger strain within the left atrium than in the proper atrium. At roughly 3 months, the valve of the oval foramen fuses with the septum secundum, forming the oval fossa (fossa ovalis). As a result, the interatrial septum becomes a complete partition between the atria. The left horn of the sinus venosus becomes the coronary sinus, and the right horn of the sinus venosus is included into the wall of the proper atrium. The the rest of the anterior internal floor of the wall of the proper atrium, as nicely as that of the proper auricle, has a rough, trabeculated look. The smooth half and rough part are demarcated internally in the proper atrium by a vertical ridge-crista terminalis, or terminal crest.
This is simply required occasionally and in considerably telescoped arches symptoms after flu shot 250mg levaquin otc, nevertheless it does necessitate a posterior strategy (preauricular or cutaneous incision) medicine to help you sleep discount levaquin express. Careful evaluation is critical medicine 853 best buy levaquin, even when not telescoped it may be bowed laterally and desires at least digital discount stroke treatment 60 minutes purchase genuine levaquin. A step-wise approach is due to this fact wanted and sufferers must give informed consent appropriately. Alternatives include the following: Isolated arch fractures 537 (a) (b) (c) (d) (e) (f) 7. Some surgeons prescribe steroids (dexamethasone/methylprednisolone) to reduce post-operative orbital swelling. This is definitely fast, however is a blind process with dangers to both eyes if incorrectly performed. As patients wake up, they may be initially agitated and the repaired web site have to be protected against inadvertent injury. Various ways of attaining this are potential, however having the site clearly marked and an alert recovery/ward nurse go a long method to (a) (b) (c) (d) 7. Swelling and bleeding behind the globe can occur, which unrecognized can lead to lack of imaginative and prescient. Careful remark of the attention is therefore necessary, a minimum of till the affected person is awake. Antibiotics and steroids could additionally be continued for a variable time and sufferers ought to be suggested not to blow their nostril. Progressive ache, deteriorating imaginative and prescient, proptosis and ophthalmoplegia are the main signs to examine. Intravenous acetazolamide, mannitol, steroids and a lateral canthotomy buy time while theatre preparations are being made. If the eyelids are swollen, gently pressing on them (not the globe) for a few minutes reduces this sufficiently to assess visual acuity. Numbness of the cheek and upper lip is an important sign that ought to generate a excessive index of suspicion for orbital or cheek bone fracture. Isolated arch or easy fractures that are incomplete on the frontozygomatic suture are those most fitted for closed discount. Correct alignment of the sphenozygomatic suture (lateral orbital wall) is a good on-table indication that the fracture is accurately decreased. Any alteration or compromise of the step-by-step surgical sequence will alter the ability to full the deliberate process and will compromise the end result. Operations are performed within the superior joint space, except disc perforations exist which allows entry into the inferior joint area. Perforation of the posterior ligament occurs in chronic dislocated discs secondary to micro- or macrotrauma. This basically includes educating the patient about limiting eccentric jaw actions, eliminating any pathologic habits, having the affected person endure Boering remedy which educates the affected person as to the character of their problem, and instructing them to take a softer food regimen and to habitually carry out nonclenching techniques. In addition, these patients should begin a regimen of oral anti-inflammatory medications to decrease any acutely inflamed course of, and wearing a soft orthotic system to both remove a bruxing habit or to soften the load positioned on the temporomandibular joints throughout bruxism. The continual bruxer can even benefit from an oral muscle relaxant to decrease the load. After two to four months of conservative therapy, the patient is re-evaluated for his or her situation. Sometimes the problem will be resolved with these measures and no further treatment is warranted. A basic distinction, however, exists in that fibrocartilage rather than hyaline cartilage lines the articular surface. This could develop primarily or as a end result of the traumatically dislocated interposing articular disc. Synovial adhesions typically accompany the medial synovial drape synovium of the posterior pouch oblique protuberance u-shape flexure of synovium anterior synovial recess anterior band of the disc lateral wall of capsule 8. Additionally, the affected person is made conscious of the possibility of seventh nerve deficits secondary to extraoral punctures, malocclusion following surgical procedure, potential scar formation from the punctures, in addition to the chance for pain, bleeding, swelling and post-operative infection. The subsequent step is making a choice on the sort of arthroscopic process the patient will obtain. The use of prophylactic antibiotics to stop post-operative an infection is controversial. The orthopaedic literature surrounding arthroscopy is scant with good potential research, for the reason that incidence for an infection following arthroscopic procedures is so low.
Buy cheapest levaquin. हैपेटाइटिस से बचाव ही इसका इलाज है | Hepatitis Symptoms and Precaution.